Other than water, coffee is the most consumed beverage in the USA. Americans drink more coffee than any other nation – over 400 million cups per day. Whether you are a die-hard coffee drinker or a casual sipper, read on for a detailed review of coffee health and performance impact, and some practical advice.
TLDR
- Beyond the stimulating effects of caffeine which can improve exercise performance, there are many health beneficial chemical compounds in coffee. These include antioxidants, minerals, pro-vitamins, and polymers which behave somewhat like other dietary fiber.
- For healthy, non-hypertensive adults, the potential heart protective benefits of coffee appear to outweigh the risks based on meta-analysis of human observational studies. Anywhere from 2-5 cups per day appears to be a sweet spot for cardiovascular disease risk reduction.
- Decaf coffee and tea offer many of the same health protective benefits of coffee if you don’t like coffee or want to reduce caffeine consumption.
- If you are attempting to reduce cholesterol by making dietary changes, swapping from unfiltered type coffees (e.g. espresso, french press) to filtered coffee might be worth exploring. Filtration will remove diterpenes, which can have a total and LDL cholesterol raising effect.
- Coffee is not an effective tool for weight loss, but may help mitigate long-term weigh gain.
- If you are interested in exploring caffeine to enhance exercise session performance, supplementation with 200-400 mg caffeine appears to be the most effective dose range for most people, taken approximately one hour before training. Personal experimentation on dose is warranted. If you choose to use coffee, a 16 oz. regular coffee is within the dosage range.
Compounds contributing to the health impacts of coffee
There are over 1,000 bioactive micronutrients in coffee. The concentration of these compounds can vary substantially depending on the beans, roasting process, and brew process. The most well-studied:
Caffeine
A stimulant of the central nervous system, caffeine indirectly affects the release of neurotransmitters which alters mood, memory, alertness, and cognitive function by blocking adenosine receptors. Caffeine content in coffee varies substantially depending on the bean and preparation method (see table at end of this post for estimated caffeine content of different coffees). Even decaf coffee has a small amount of caffeine.
Chlorogenic Acids (CGAs)
CGAs are a subset of naturally occurring polyphenolic compounds found in coffee beans and many other plants. Metabolized products of CGAs can induce antioxidant and anti-inflammatory effects. In espresso or other higher-pressure extraction processes such as a moka pot, CGA content can be much higher due to the larger amount of coffee is used per volume of water versus brews prepared by drip filter. CGA content will also be higher with beans that are lighter roasted. Generally, cold brews with short infusion periods and lower temperatures tend to yield lower CGA levels.
Melanoidins
Melanoidins are polymeric compounds formed during the coffee bean roasting process from a reaction of carbohydrates, amino acids, and phenolic compounds. They contribute to the sensorial properties of coffee via the Maillard reaction which is the thermal process of “browning” (the same is responsible for the crust on bread, searing on steak). A diet rich in coffee, bread, and cereals can provide up to 10g of melanoidin per day. Interestingly, melanoidins seem to act much like dietary fiber in the colon and contribute to gut health.
Cafestol and Kahweol
Cafestol and Kahweol are esterified fatty acid compounds that impart some of the oily texture of coffee. These compounds are retained in unfiltered coffee, but largely removed in filtered coffee. Cafestol and Kahweol can have total and LDL cholesterol raising effects, but on the other hand also demonstrate potentially beneficial anti-inflammatory and anticarcinogenic activity. Further research is needed on the pharmacological properties of these compounds.
Trigonelline
A vitamin B3 (niacin) precursor that gives coffee some of its bitter taste and can help upregulate our antioxidant defense system. Trigonelline may have therapeutic potential as a hypoglycemic, neuroprotective, and anticarcinogenic agent per rodent models and limited studies. More research in the area is required to better elucidate the action of trigonelline within coffee.
Minerals
The mineral content in coffee varies considerably depending on the bean, brew method, and of course the water source. A review of research spanning 2000 – 2020 notes that one portion of coffee brew can cover 7.5% or 6.4% (for women and men) and 6.6% of the daily requirement for magnesium and potassium, respectively. Coffee provides slightly lower amounts of phosphorus (up to 2.2%), sodium (up to 2.2%), and calcium (up to 0.7% of the daily requirement for women and 0.6% for men).1
Coffee and Cardiovascular Disease (CVD)
A dose-response meta-analysis of observational, prospective cohort studies (35 studies comprising 1,283,685 participants analyzed) conducted by Ding et. al indicates a J-shaped non-linear relationship between coffee consumption and risk of CHD and stroke.2 cardiovascular disease (CVD), with modest effect. Lowest risk was associated with consumption of 3-5 cups/day.
The “J-shape” of the curve likely reflects a combination of beneficial and detrimental effects. For moderate coffee consumption; beneficial effects may be greater than adverse effects; whereas for heavy consumption, detrimental effects may counterbalance beneficial effects.
Association of Coffee Consumption with CVD risk reduction.2

No association was found with decaffeinated coffee and CVD risk, however this may be related to reverse causation (people with CVD-related conditions may switch from regular coffee to decaf), or that the overall consumption of decaffeinated coffee is much lower than caffeinated coffee, providing a less significant pool of data. It’s also worth noting that tea consumption (3 cups/day) is associated with reduced risk of coronary heart disease.3
Another meta-analysis regarding the association between habitual coffee consumption and heart failure risk found that 3-4 servings of coffee/day provided the strongest risk reduction.4
There does not appear to be a significant dependency on age. Certain previous studies in the scientific literature conflict with these findings.5 However, these studies do not appear to have risk-adjusted for enough cofounding health-related variables. Given the effect size of coffee on CVD risk is only mild to moderate, it stands to reason that statistical adjustments and assumptions within individual studies can lead to divergent findings.
Coffee and Blood Pressure
Light to moderate coffee (and tea) consumption is likely to confer some cardiovascular protective benefit in non-hypertensive individuals.
Coffee can acutely raise blood pressure by the action of caffeine, more notably in individuals who are not habituated to caffeine. These effects are typically transient, with blood pressure returning to normal level within a few hours. A recent metanalysis found no long-term blood pressure raising effects of coffee.6 A large prospective study in non-hypertensive female nurses found that coffee consumption mildly reduced risk hypertension risk.7
Although caffeine has an acute hypertensive effect, the other active compounds found in coffee in tea may have an anti-hypertensive effect (such as chlorogenic acids, soluble fiber, and potassium) which could exert a beneficial effect in the cardiovascular system. Green and black tea has also been shown to reduce blood pressure for individuals who are pre-hypertensive or hypertensive.8
A number of compounds in coffee and tea can work as long-term anti-hypertensive agents, but because people with hypertension are more susceptible to the effects of caffeine, caffeine’s harmful effects may outweigh its protective effects and increase the risk of mortality in people with severe hypertension.
Heavy coffee consumption was associated with an increased risk of CVD mortality among people with severe hypertension,9 but not people without hypertension. In contrast, green tea consumption was not associated with an increased risk of CVD mortality across all categories of blood pressure. Although the precise nature of the relation between coffee and blood pressure is still unclear, most evidence suggests that regular intake of caffeinated coffee does not increase the risk of hypertension, in non-hypertensive individuals.
Coffee and Type 2 Diabetes (T2DM)
Chlorogenic acids can reduce fasting plasma glucose concentrations, increase sensitivity to insulin, and slow the appearance of glucose in circulation after a glucose load. A systematic review of nine cohort studies compared minimal to low coffee consumption (<2 cups/day) with that of heavy coffee consumption (>6 cups/day) for the risk of the development of type 2 diabetes mellitus (T2DM). The study concluded that the risk of the development of T2DM was lowest in subjects who drank >6 cups daily but also significantly reduced in subjects who consumed 4-6 cups per day.10 A prospective study of >88,000 women 26 to 46 years of age established a linear relationship of coffee consumption with the reduction in T2DM, whereby even small amounts of daily coffee conferred benefit. Associations were similar for noncaffeinated and caffeinated coffee.11
Green tea consumption has also been shown to reduce the risk of T2DM, which is possibly mediated through the antioxidant and anti-inflammatory effects of catechins. A 2020 meta-analysis showed that green tea significantly reduces the incidence of T2DM; however black tea did not. The authors concluded that different types of tea have varying protective mechanisms on metabolic syndrome although the explanation for this observation is unclear.12
Coffee (and green tea) may have protective benefits against T2DM, and this seems to be independent of caffeine content.
Coffee and Cholesterol
Contributing to the bitter taste of coffee, cafestol and kahweol are natural diterpene fatty esters extracted from coffee beans, and the concentrations of these compounds is strongly influenced by the preparation method. They are present are present in larger amounts in unfiltered coffee such as Turkish coffee, cold press, and espresso. They are mostly removed when coffee is filtered, or during processing in the case of instant coffee.
A meta-analysis of 14 randomized controlled trials examining the effect of coffee consumption on serum cholesterol concentrations indicate that the consumption of boiled coffee dose-dependently is associated with higher serum total and LDL cholesterol concentrations, while the consumption of filtered coffee results in slight increase in serum cholesterol.13 Cafestol seems to be the more potent actor in elevation of serum cholesterol.
While Cafestol and Kahweol may increase total and LDL cholesterol, these compounds also enhance our built-in antioxidant defense system against oxidative damage and inflammation.
If you drink unfiltered coffee and are actively trying to reduce your cholesterol, consider swapping to filtered coffee. If your cholesterol is normal, there’s no strong long-term evidence of chronic elevation of serum lipids or negative outcomes associated with this elevation.
Coffee Impact on Weight and Appetite
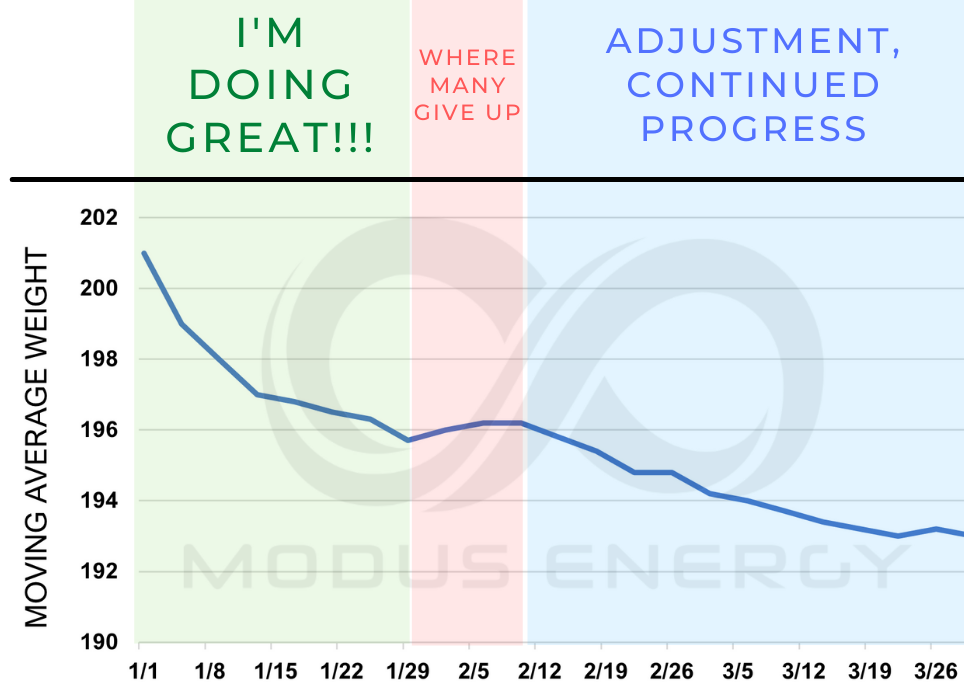
Studies to date indicate a very small but not insignificant association between coffee consumption and suppression of fat accumulation leading to lower long term weight gain.14, 15, 16 To understand how coffee can potentially mitigate weight gain, consider the action of the constituents:
Coffee’s potential impact on energy expenditure
Caffeine elicits thermogenesis (production of body heat), increases the energy cost of movement resulting in increased total daily energy expenditure, resting metabolic rate, and exercise activity expenditure. The impact appears to be dose dependent, even caffeine doses of 100 mg can induce an increase in resting metabolic rate of 3-4%. The magnitude of energy expenditure increases near linearly with caffeine quantity; doses of 200-250 mg increases RMR by 10-12%. For reference, a 5% increase in RMR within a 24-hour period represents and additional expenditure of 75-100 kcal/day depending on the individual (it appears that dosage should be based on body weight versus absolute values). This may seem like a small number, but accumulated over weeks, months, and years it is a viable hypothesis for caffeine to mitigate weigh gain over time.
A 2023 prospective cohort study investigated coffee consumption and weight gain. Increase in intake of unsweetened caffeinated and decaffeinated coffee was inversely associated with weight gain, and each 1 cup per day increment in unsweetened caffeinated coffee was associated with a reduction in 4-y weight gain of -0.12 kg. The addition of sugar to coffee counteracted coffee’s benefit for possible weight management.17
Coffee’s potential impact on energy intake and appetite control
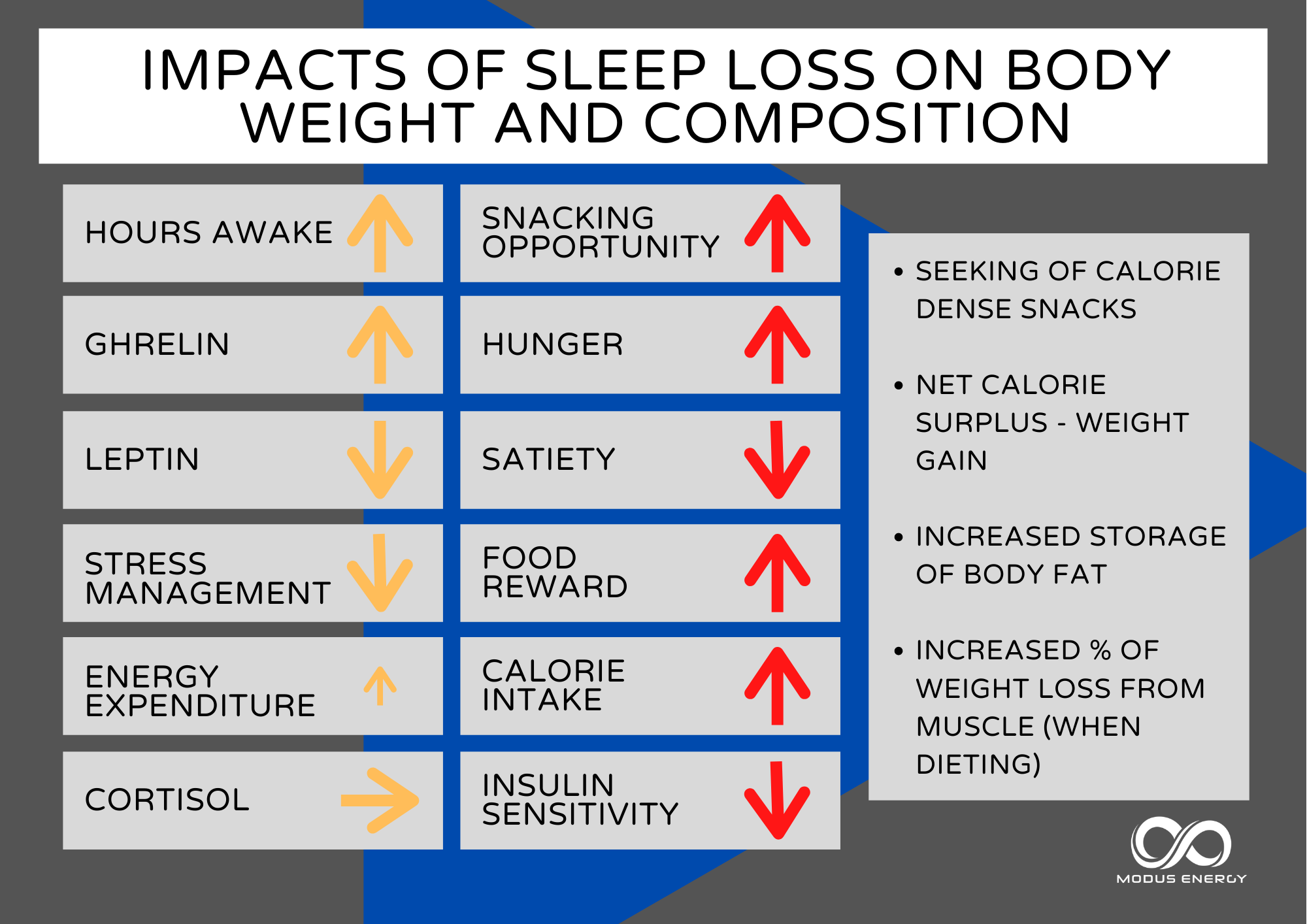
The impact of coffee on intake and appetite is not clear. There are some plausible mechanisms by which coffee could potentially reduce energy intake or appetite. Compounds in coffee could decrease the rate of gastric emptying, causing food to stay in your stomach longer promoting satiety. Coffee could alter the secretion of certain hormones, specifically 1) downregulating ghrelin (a gastric hormone that stimulates appetite, 2) upregulating PYY (released in the intestinal tract to suppress hunger), 3) upregulating leptin a hormone released mainly from fat cells which supports feeling of satiety. Caffeine specifically could reduce appetite by increasing the release of adrenaline and cortisol. On the other hand, some report appetite stimulation from caffeine.
Very few studies that have examined caffeinated coffee consumption reduces appetite and energy intake, and those that are available are contradictory in their results. In a small, limited study decaffeinated coffee yielded significantly subjective lower hunger during the whole 180- minute study period and higher plasma PYY for the first 90 minutes versus water placebo.18 Caffeine in water had no effects on hunger or PYY. Caffeinated coffee showed a pattern between that of decaffeinated coffee and caffeine in water. There were no significant changes in ghrelin or leptin. In another limited study, a moderate coffee amount (2- 4 cups, 6 mg/kg body weight reduced reduce energy intake in the following meal and in the total day compared to lower or no coffee intake in overweight/obese participants but had no impact on normal-weight individuals.19
One rodent model study may provide us some understanding of complex nature of the relationship between caffeine and hunger.20 Caffeine administered acutely to mice at moderate to high doses can increase binge eating when the subjects had already stablished a pattern of excessive eating. However, this same dose led to clear reductions in food consumption if the mice were in an environment promoting high anxiety levels. Another consideration is fatigue – one the effects of caffeine wear off; appetite may be stimulated due to tiredness.
Coffee may help prevent weight gain through the action of a number of its constituents including caffeine, but it’s not a good as a primary strategy for weight loss. Assess personally if coffee helps take the edge off hunger, or if it makes you prone to eat more under certain circumstances.
Coffee and Athletic Performance
Caffeine: supplementation with caffeine can provide a degree of performance benefit, most notably increase time to exhaustion when aerobic and muscular endurance or is required,21 or sleep deprivation is considered. Effective dosages typically fall within the range of 3-6mg/kg of body weight22 – this is about 200 – 400 mg for a 150 lb. individual. It takes some experimenting to find the appropriate personalized dosage as some are more sensitive to caffeine than others. The recommended timing for ingestion is about one hour before exercise.
As a reference, here is the average caffeine content of different coffees, normalized per fluid ounce and then reported on a typical serving basis. Note that the values reported here are averages – caffeine content can vary *substantially* by coffee bean type and brewing conditions.
Caffeine Content in Coffee and Tea

Regarding the role of chlorogenic acids and other bioactive compounds to mitigate oxidative stress (protein, lipid, and DNA damage) and mediate antioxidant capacity, data is limited and results are conflicting related to the lack of control on types of coffee and dosage, brew procedures as well as biomarker test methodology.
Hope you found this post informative! Reach out anytime with questions.
Instagram: @kmcgrath.phd Facebook: @1modusenergy

Ready to start?
Get started with nutrition coaching
1. Olechno E, Puścion-Jakubik A, Socha K, Zujko ME. Coffee Brews: Are They a Source of Macroelements in Human Nutrition? Foods. 2021 Jun 9;10(6):1328. doi: 10.3390/foods10061328.
2. Ding M, Bhupathiraju SN, Satija A, van Dam RM, Hu FB. Long-term coffee consumption and risk of cardiovascular disease: a systematic review and a dose-response meta-analysis of prospective cohort studies. Circulation. 2014 Feb 11;129(6):643-59.
3. Zhang C, Qin YY, Wei X, Yu FF, Zhou YH, He J. Tea consumption and risk of cardiovascular outcomes and total mortality: a systematic review and meta-analysis of prospective observational studies. Eur J Epidemiol. 2015 Feb;30(2):103-13.
4. Mostofsky E, Rice MS, Levitan EB, Mittleman MA. Habitual coffee consumption and risk of heart failure: a dose-response meta-analysis. Circ Heart Fail. 2012 Jul 1;5(4):401-5.
5. Liu J, Sui X, Lavie CJ, Hebert JR, Earnest CP, Zhang J, Blair SN. Association of coffee consumption with all-cause and cardiovascular disease mortality. Mayo Clin Proc. 2013; 88:1066–74.
6. Han M, Oh Y, Myung SK. Coffee Intake and Risk of Hypertension: A Meta-Analysis of Cohort Studies. J Korean Med Sci. 2022 Nov 21;37(45):e332.
7. Winkelmayer WC, Stampfer MJ, Willett WC, Curhan GC. Habitual caffeine intake and the risk of hypertension in women. JAMA. 2005 Nov 9;294(18):2330-5.
8. Yarmolinsky J, Gon G, Edwards P. Effect of tea on blood pressure for secondary prevention of cardiovascular disease: a systematic review and meta-analysis of randomized controlled trials. Nutr Rev. 2015 Apr;73(4):236-46.
9. Teramoto M, Yamagishi K, Muraki I, Tamakoshi A, Iso H. Coffee and Green Tea Consumption and Cardiovascular Disease Mortality Among People With and Without Hypertension. J Am Heart Assoc. 2023 Jan 17;12(2):e026477. doi: 10.1161/JAHA.122.026477.
10. Huxley R, Lee CM, Barzi F, et al. Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Arch Intern Med 2009;169:2053–63.
11. van Dam RM, Hu FB. Coffee consumption and risk of type 2 diabetes: a systematic review. JAMA 2005;294:97–104.
12. Liu W , Wan C , Huang Y , Li M . Effects of tea consumption on metabolic syndrome: a systematic review and meta-analysis of randomized clinical trials. Phytother REs 2020;34(11):2857–66 .
13. Jee SH, He J, Appel LJ, Whelton PK, Suh I, Klag MJ. 2001. Coffee consumption and serum lipids: a meta-analysis of randomized controlled clinical trials. Am J Epidemiol 153:353–362.
14. Larsen SC, Mikkelsen ML, Frederiksen P, Heitmann BL. Habitual coffee consumption and changes in measures of adiposity: a comprehensive study of longitudinal associations. Int J Obes (Lond). 2018 Apr;42(4):880-886.
15. Nordestgaard AT, Thomsen M, Nordestgaard BG. Coffee intake and risk of obesity, metabolic syndrome, and type 2 diabetes: a Mendelian randomization study. Int J Epidemiol 2015; 44: 551–565.
16. Lopez-Garcia E, van Dam RM, Rajpathak S, Willett WC, Manson JE, Hu FB. Changes in caffeine intake and long-term weight change in men and women. Am J Clin Nutr 2006; 83: 674–680.
17. Henn M, Glenn AJ, Willett WC, Martínez-González MA, Sun Q, Hu FB. Changes in Coffee Intake, Added Sugar and Long-Term Weight Gain – Results from Three Large Prospective US Cohort Studies. Am J Clin Nutr. 2023 Dec;118(6):1164-1171.
18. Greenberg JA, Geliebter A. Coffee, hunger, and peptide YY. J Am Coll Nutr. 2012 Jun;31(3):160-6.
19. Gavrieli A, Karfopoulou E, Kardatou E, Spyreli E, Fragopoulou E, Mantzoros CS, Yannakoulia M. Effect of different amounts of coffee on dietary intake and appetite of normal-weight and overweight/obese individuals. Obesity (Silver Spring). 2013 Jun;21(6):1127-32.
20. Correa M, SanMiguel N, López-Cruz L, Carratalá-Ros C, Olivares-García R, Salamone JD. Caffeine Modulates Food Intake Depending on the Context That Gives Access to Food: Comparison With Dopamine Depletion. Front Psychiatry. 2018 Sep 6;9:411.
21. Wang Z, Qiu B, Gao J, Del Coso J. Effects of Caffeine Intake on Endurance Running Performance and Time to Exhaustion: A Systematic Review and Meta-Analysis. Nutrients. 2022 Dec 28;15(1):148.
22. Guest NS, VanDusseldorp TA, Nelson MT, Grgic J, Schoenfeld BJ, Jenkins NDM, Arent SM, Antonio J, Stout JR, Trexler ET, Smith-Ryan AE, Goldstein ER, Kalman DS, Campbell BI. International society of sports nutrition position stand: caffeine and exercise performance. J Int Soc Sports Nutr. 2021 Jan 2;18(1):1.
I am an Amazon Associate and can earn fees on purchases. This helps keep the website ad-free.